Consider this a friendly consult in print. We’ll unpack six bariatric procedures offered statewide and share real-world weight-loss stats, transparent prices, and altitude-specific risks.
Why surgery? Diets, apps, and GLP-1 drugs usually top out around 15 percent total-body loss, while operations average 25–30 percent and often send diabetes into remission. Colorado law also forces insurers to cover proven options when you meet NIH criteria.
Ready to match a procedure to your BMI, budget, and lifestyle? Let’s dive in.
What’s different about choosing surgery in Colorado?
Colorado offers genuine home-court advantages and just a couple of quirks you should know about.
First, access is wide-open. Six MBSAQIP-accredited programs stretch from Denver to Colorado Springs, so you can book consults without leaving the state.
Elevation creates the only notable wrinkle. A 2021 multicenter study in Surgery for Obesity and Related Diseases reported that sleeve patients treated above 5,000 feet saw about a two-times higher blood-clot rate than peers at sea level; local surgeons counter this with extended blood-thinner regimens and early-walking plans, keeping overall complication numbers low.
Coverage tilts in your favor too. Colorado law requires marketplace insurers, plus Medicaid, to pay for proven bariatric procedures once you meet NIH criteria. Programs must also publish package prices up front, which eliminates “mystery bill” anxiety.
One standout is the Bariatric & Metabolic Center of Colorado in Parker—an MBSAQIP-accredited site whose 2026 rate sheet lists a self-pay gastric sleeve at $12,250, an all-inclusive bundle covering the surgeon, anesthesia, up to a two-night stay, and 90 days of follow-up visits.
Eligibility is spelled out plainly: the center’s Bariatric surgery FAQs note that a BMI above 40—or 35 when paired with issues like diabetes—usually meets insurer criteria, and they place sleeve risk on par with routine gallbladder surgery, adding context to why this price tag draws so many locals.
Bottom line: you can shop locally, compare posted prices, and trust that every care team already builds altitude precautions into the plan—so you can focus on choosing the best procedure, not the best ZIP code.
How we judge “best” when options are so different
Choosing a weight-loss procedure is not like picking between six flavors of the same drink. Each surgery alters anatomy, appetite, and daily routine in its own way. To keep comparisons fair, we measure every option against six yardsticks.
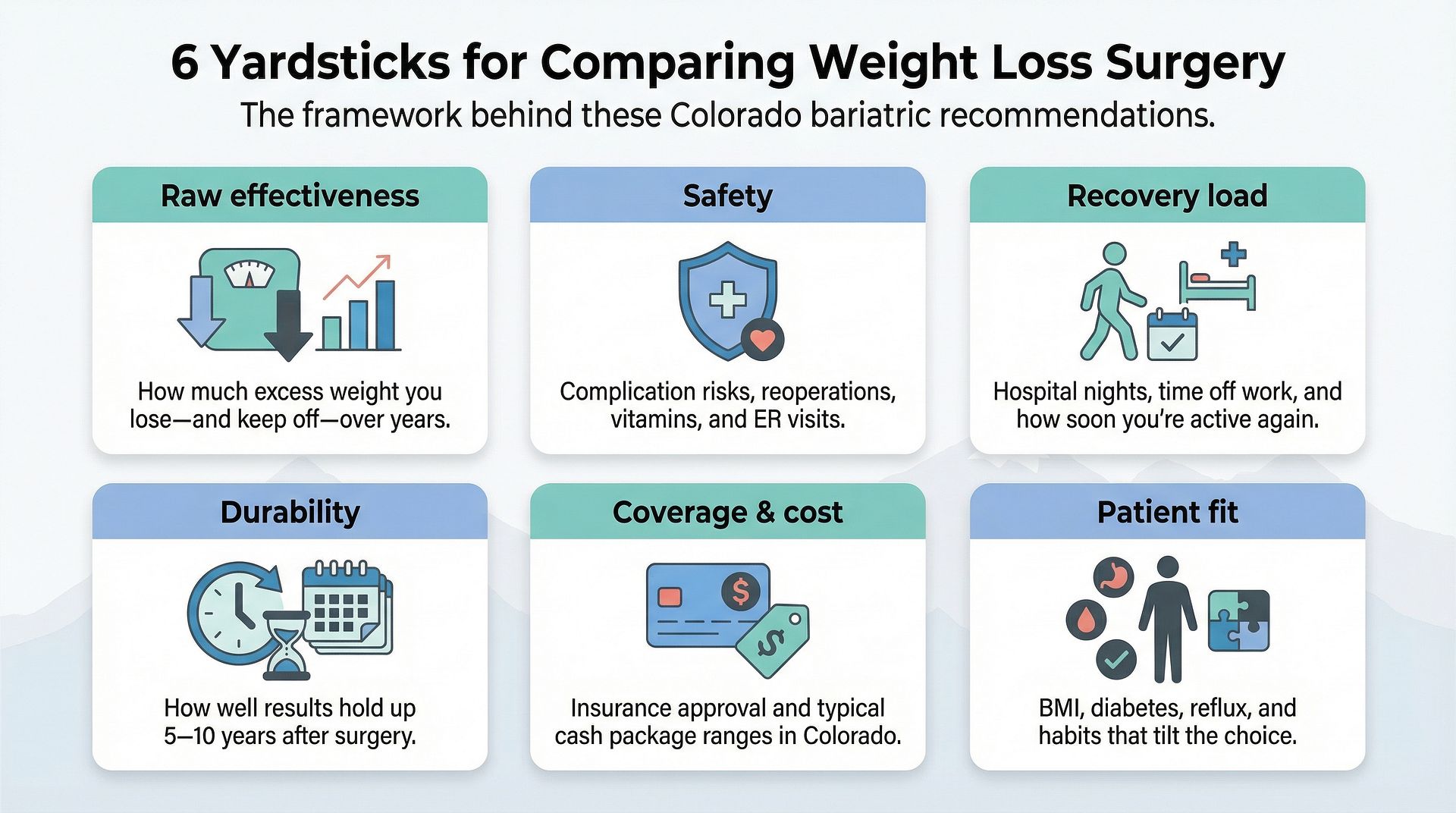
- Raw effectiveness. We track the percent of excess weight patients lose in the first year and how much stays off five years later. Data outranks anecdotes.
- Safety. Every operation here is laparoscopic or endoscopic, yet complication rates still differ. We flag issues that may require another surgery, lifelong vitamin therapy, or unexpected ER visits.
- Recovery load. Nights in the hospital, when you can drive, and how soon you can hike again all matter when Colorado weekends call.
- Durability. A sleeve or bypass is permanent; a balloon leaves at month six. We show what that means for weight control a decade out.
- Coverage and cost. Colorado insurers often cover the three primary surgeries but rarely the newer endoscopic tools. We share typical cash prices so you can budget before the first lab draw.
- Patient fit. BMI, diabetes status, reflux history, and even snack habits tilt the choice toward one procedure or another.
Keep these six yardsticks in mind; they turn a crowded menu into a focused short list built around you.
Gastric sleeve surgery: Colorado’s go-to option
Picture your stomach as a football. During a sleeve, surgeons remove the laces and most of the leather, leaving a slim banana-shaped tube that fills quickly and empties slowly.
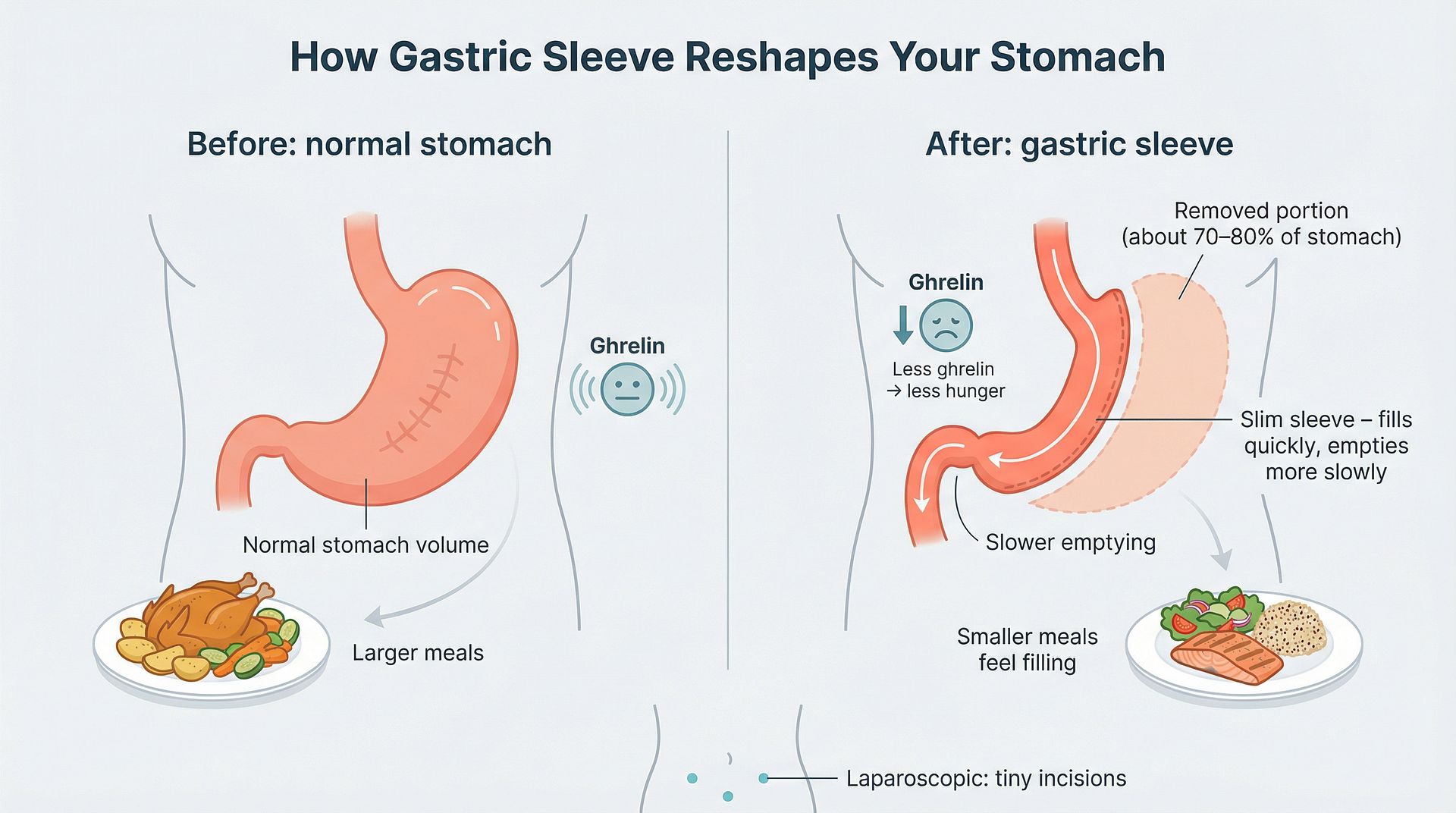
That single change packs a double punch: smaller portions and lower ghrelin, the “feed me” hormone. Most Colorado patients lose about 65 percent of excess weight within 12–18 months and keep roughly 55 percent off long-term, a sweet spot between sizable results and manageable risk.
Safety strengthens the appeal. The sleeve is laparoscopic, usually three small incisions, and many centers discharge healthy adults the morning after surgery. Staple-line leaks run under three percent at accredited programs, on par with gallbladder removal.
Daily life stays simple. You digest food normally, so vitamin needs are lighter than with a bypass or switch. You will still take supplements and focus on protein, but malabsorption does not enter the worry list.
Cost and coverage close the deal. Nearly every major insurer in Colorado approves sleeves for a BMI ≥ 40, or 35 with a related disease. Paying cash? Published packages range from $12,000 to $20,000, often bundled with six months of nutrition coaching.
The main caveat is reflux. If you battle heartburn now, talk with your surgeon; a sleeve can turn mild GERD into a nightly visitor. Otherwise, for many Coloradans, the sleeve offers the strongest mix of effectiveness, safety, and convenience in 2026.
Gastric bypass surgery: the heavyweight for diabetes and reflux
A bypass is a two-step redesign. Surgeons create a thumb-sized pouch at the top of the stomach, then route part of the small intestine to that pouch. Food skips roughly four feet of gut, so you feel full fast and absorb fewer calories.
Results arrive quickly. Colorado data show 70–80 percent of excess weight gone within 18 months. More striking, 60 percent of people with type 2 diabetes leave the hospital off insulin and stay in remission for years.
This powerhouse also tames severe heartburn. Acid cannot back-flow into a pouch that holds only three bites, so many long-time GERD sufferers call bypass their cure.
Trade-offs are real. The reroute blocks key absorption sites, so lifelong vitamins—B-12, iron, calcium—become standard. Eat concentrated sugar and “dumping,” a sweaty, dizzy sprint for the couch, may follow; some see it as built-in candy control.
Surgery time sits near two hours, and most patients spend two nights at an MBSAQIP center. Complication rates stay low in high-volume programs, yet leaks or internal hernias, though rare, carry heftier consequences than sleeve issues.
On cost, published cash packages run $18,000–$25,000, and insurers routinely approve bypass for BMI ≥ 40 or 35 with serious comorbidities. Many endocrinologists steer their hardest-to-control patients toward this option first.
Choose bypass for maximum weight loss, diabetes freedom, and reflux relief if you are ready to stick with the vitamin regimen that secures those wins.
Duodenal switch (and SADI-S): the max-loss option for super obesity
Think of the duodenal switch as a two-for-one procedure: surgeons first create a gastric sleeve, then reroute the small intestine much lower than a bypass. The combo delivers fierce portion control plus major calorie malabsorption.
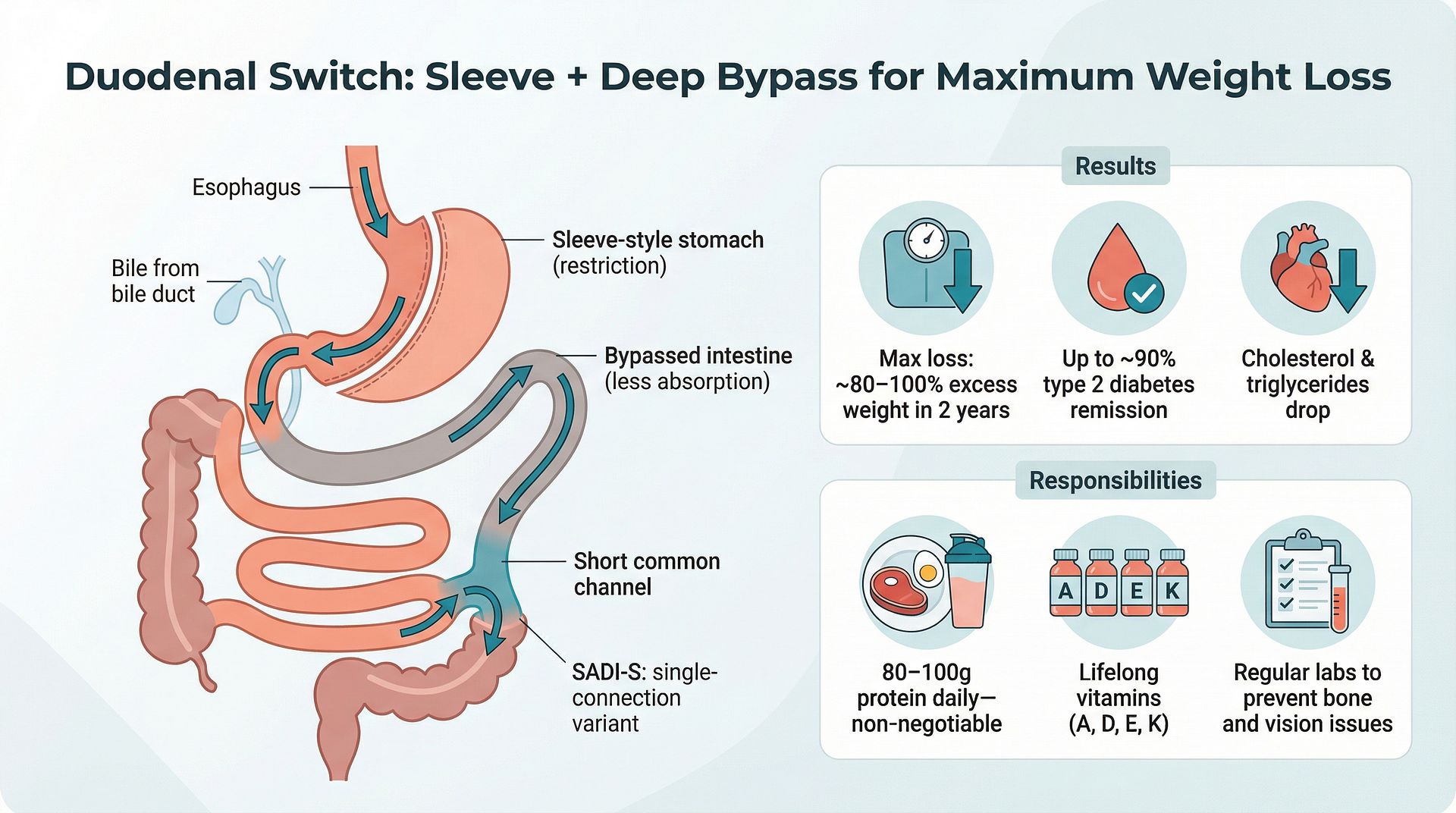
Because of that pairing, Colorado registry data show patients lose 80–100 percent of excess weight within two years. Many reach a normal BMI for the first time since childhood.
Metabolic payoffs match the scale of weight loss. Up to 90 percent of people with stubborn type 2 diabetes move into full remission, while cholesterol and triglycerides plunge as fat absorption drops.
Power, however, comes with strings. Hitting 80–100 grams of protein daily and taking a pharmacy’s worth of fat-soluble vitamins for life is non-negotiable. Skipping labs can let deficiencies such as night-blindness or bone loss creep in.
Surgery runs three to four hours and usually requires two nights in hospital. Only a handful of high-volume Colorado surgeons perform the switch or its single-anastomosis cousin, SADI-S, so travel to Denver or Parker is common.
Cash packages sit around $20,000–$30,000, and most insurers approve the switch only for BMI ≥ 50 or after a prior procedure fails. If you want the biggest hammer and are prepared for disciplined follow-up, the duodenal switch offers unrivaled weight loss.
Adjustable gastric band: once popular, now a niche choice
The idea sounds elegant: slip a silicone band around the top of the stomach, inflate it like a cuff, and tighten hunger on demand. Real-world results tell a different story.
Registry data from the American Society for Metabolic and Bariatric Surgery show less than 50 percent excess-weight loss, and nearly 33 percent of Colorado patients have the band removed within five years because of slippage, erosion, or poor tolerance. Many then convert to a sleeve or bypass, adding another operation to the journey.
Same-day discharge is common, and the band is fully reversible. Long-term life can be fussy, with regular office fills, surprise vomiting if bites are too big, and nighttime reflux when the band sits too tight. Success depends on meticulous chewing and frequent tweaks.
Coverage is fading as insurers follow the high revision rate. Paying cash? Placement averages $10,000–$15,000, and follow-up adjustments often carry extra fees.
Who still fits the band? A small group with lower BMI who reject permanent anatomy changes and commit to close follow-up. For most others, newer procedures deliver more weight loss with fewer maintenance headaches.
Endoscopic sleeve gastroplasty (ESG): surgery-like results without incisions
ESG trims stomach volume with sutures placed through a flexible scope passed down the throat. No cuts, no scars, and most people head home the same day.
Volume drops about 70 percent, so meals feel Thanksgiving-full after a few bites. Early registry data show approximately 15 percent total-body weight loss at one year—roughly half of a surgical sleeve but three to four times better than diet alone.
Recovery moves quickly. Many Colorado clients resume remote work inside two days and return to light workouts by week two. Nausea and cramps usually fade within 72 hours.
Because intestines stay intact, vitamin shortages are uncommon. ESG is also reversible; stitches can be released later, although that request is rare.
Cost is the main hurdle. Insurers still list ESG as investigational, so expect self-pay packages of $9,000–$15,000. Clinics often include a year of nutrition coaching and an optional “tightening” session if the sleeve loosens.
Who benefits most? Adults with BMI 30–40 who prefer a powerful tool without permanent surgery, busy professionals who cannot spare hospital nights, and patients eyeing a future surgical sleeve who first aim to lose 30–50 pounds to lower operative risk.
Intragastric balloon: a 6-month kick-start, not a forever fix
During a brief endoscopy, the care team slips a soft balloon into the stomach and fills it with saline. The device floats for six months, hogging space and slowing gastric emptying so you feel full on kid-sized portions.
Clinical trial summaries report 10–15 percent total-body weight loss by the time the balloon comes out. That drop can ease borderline diabetes or prepare you for a later sleeve, though it falls well below surgical numbers.
The first week can be rough. Roughly 20 percent of patients battle intense nausea or vomiting; a small group requests early removal. After that, most people adjust to smaller meals and steady loss.
Because the balloon exits at month six, the real test starts then. Without firm nutrition coaching, weight often creeps back. Colorado programs bundle a full year of dietary support to lock new habits before removal.
Insurance rarely covers the balloon, so budget $6,000–$9,000 out of pocket. The upside is minimal downtime; many people return to work within 24–48 hours, and there are zero anatomy changes.
Choose a balloon if your BMI sits near 30–35, you want a short-term boost, and you are disciplined about lifestyle work once the training wheels come off.
How the six options stack up, side by side
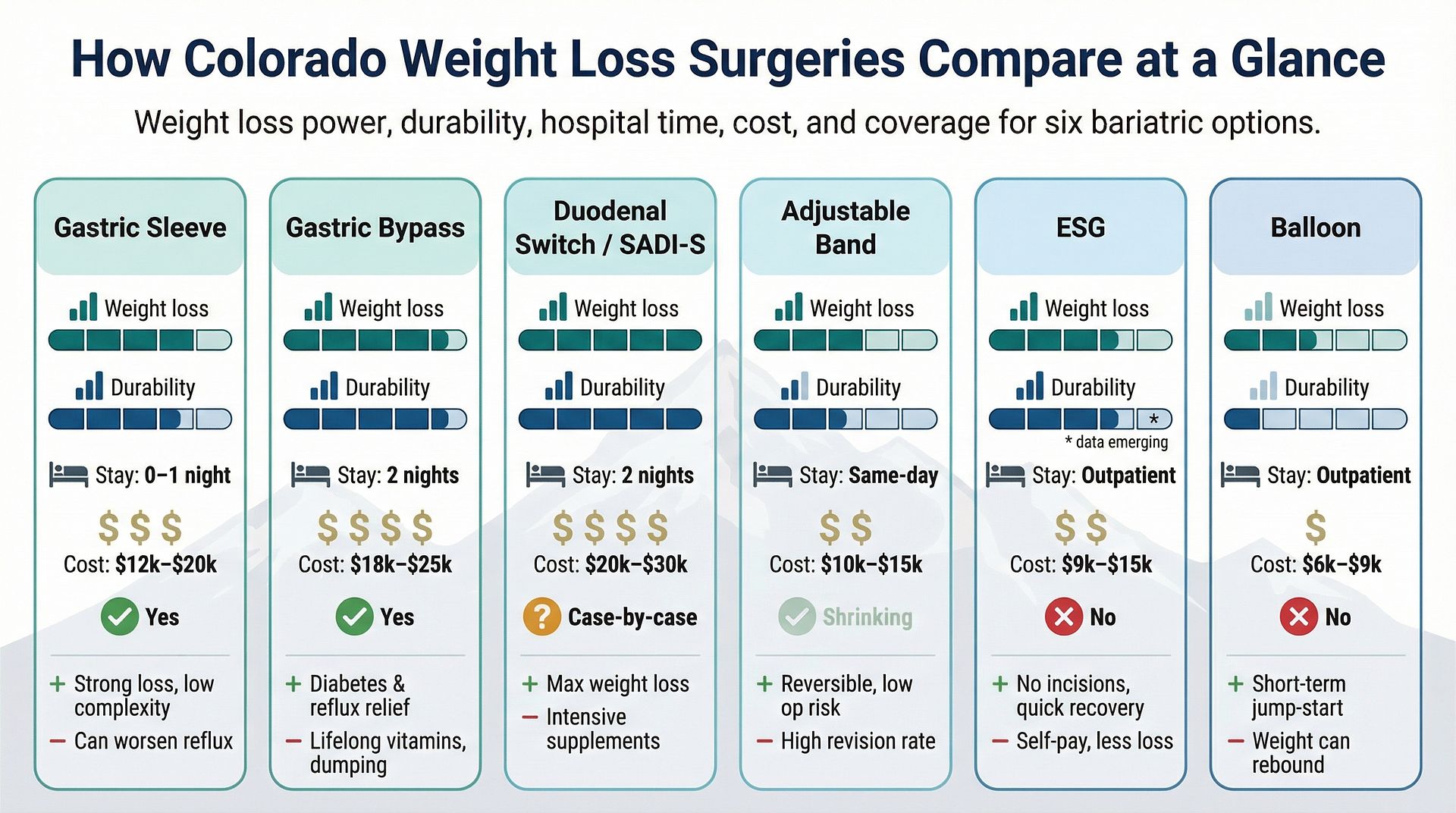
| Procedure | 1-year excess-weight loss | 5-year durability | Hospital stay | Typical cash cost (CO) | Insurance coverage | Key upside | Biggest watch-out |
| Gastric sleeve | ~65% | ~55% | 0–1 night | $12k–$20k | Yes | Strong loss, low complexity | Can worsen reflux |
| Gastric bypass | 70–80% | ~60% | 2 nights | $18k–$25k | Yes | Diabetes and GERD relief star | Lifelong vitamins plus dumping |
| Duodenal switch / SADI-S | 80–100% | 75–85% | 2 nights | $20k–$30k | Case-by-case | Max weight loss | Intensive supplement load |
| Adjustable band | 40–50% | 25–30% | Same-day | $10k–$15k | Shrinking | Reversible, low op risk | High revision rate |
| ESG | 50–60% (EWL) | 30–50%* | Outpatient | $9k–$15k | No | No incisions, rapid recovery | Self-pay, less loss |
| Balloon | 20–30% (EWL) | Temporary | Outpatient | $6k–$9k | No | Quick jump-start | Weight can rebound |
*Five-year data still emerging.
Conclusion
Keep three points in mind while scanning:
- Percentages refer to excess weight, not total. Losing 60 percent of 100 excess pounds equals 60 pounds lost.
- Cash prices are bundled estimates from Colorado programs posting public rates in 2026; your quote may vary with extra tests or longer follow-up.
- Coverage hinges on BMI and comorbidities. Verify payer requirements before scheduling labs.



